

India’s teenage motherhood crisis is not just about early pregnancy – it is about how poverty, anaemia, lack of nutrition, and early marriage combine to shape the lives of both young mothers and the children they raise. Using data from the National Family Health Survey (NFHS-5), the article shows that millions of adolescent girls in India still begin childbearing while they are physically, emotionally, and socially unprepared for motherhood.
A girl who becomes a mother at 16 is still a child herself. What NFHS-5 tells us about the compounding disadvantages she and her child will carry. Almost 6.8% of girls between 15 and 19 years in India have already begun childbearing, meaning they are either pregnant or have given birth. According to Asian Journal of Population Sciences 2023, this amounts to about one in fifteen teenage girls. In states like Tripura, the figure rises to 21.9%. In West Bengal, Jharkhand, and Bihar, the number remains stubbornly high. This statistic has improved over time. In NFHS-3 (2005-06), it was at 16%; this decline is real and should be recognised.
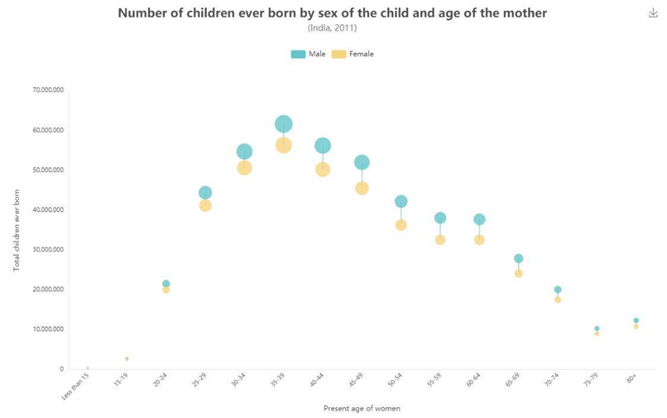
However, the overall figure is still significant. With India’s adolescent population exceeding 250 million, a 6.8% rate translates to millions of young girls facing pregnancy, delivery, and early motherhood often while still adolescents themselves, frequently anaemic, with limited formal education, and almost always lacking adequate institutional support.
Source: Census India
What the data highlights and the impact on the child being raised by these young mothers.
Before looking at how teenage motherhood affects child development, it’s important to understand who these girls are and the circumstances surrounding their pregnancies. NFHS-5 data states that teenage childbearing in India mainly reflects poverty, caste, and early marriage. Education is another key factor that impacts the young mother. According to NFHS-5, among girls with no schooling, 18% have begun childbearing by ages 15-19. In contrast, just 4% of girls with 12 or more years of education have started childbearing. Education is not only associated with delayed childbearing; it serves as a protective factor.
Financial ability tells a similar story. Only 2% of teenage girls in the highest wealth quintile have begun childbearing, compared to 10% in the lowest quintile. The disparity is steep and consistent. Caste and community influence outcomes as well. Teenage childbearing rates are highest among Scheduled Tribes at 8.7%, followed by Scheduled Castes at 7.3% and other caste groups at 7%. These differences are significant.
Marriage is the most direct pathway. More than 53% of currently married girls aged 15-19 have begun childbearing compared to significantly lower rates among unmarried adolescents. In India, unlike many Western countries, adolescent pregnancy mainly results from early marriage rather than from unmarried sexual activity. This distinction is crucial for policy: reducing teenage pregnancy in India requires delaying marriage, not just promoting contraception.
A Body Not Yet Ready
A teenage girl’s body is still growing. Pregnancy at this age carries serious physiological risks that are well-documented.
Anaemia is perhaps the most pressing issue. NFHS-5 shows that 59.1% of adolescent girls (15-19 years) are anaemic—the highest rate among any demographic group in the survey. This figure worsened from NFHS-4 to NFHS-5, rising from 54% to 59.2%, even while the government’s Anaemia Mukt Bharat program was in effect. Twenty-one of 28 states reported an increase.
An anaemic adolescent who becomes pregnant enters a difficult situation. Anaemia during pregnancy increases the risk of maternal mortality, preterm birth, low birth weight, and—critically—anaemia in the newborn. The mother’s nutritional deficit becomes the child’s starting point before the child has taken a single breath.
Child mortality data show a similar pattern. According to NFHS-5, Children born to mothers under 20 have a mortality rate of 53 deaths per 1,000 live births, significantly higher than for children born to older mothers. Children of teenage mothers are more likely to be underweight at birth, more likely to be stunted, and more likely to suffer the consequences of early-life nutritional deprivation as they grow up.
Stressed Mother and Developing Brain
The conversation often stops here. Maternal health indicators get measured and debated, while what happens after delivery during the early stages of caregiving receives much less attention. This gap is critical because the first three years of a child’s life are when the most important brain development occurs. The neural pathways established during this time through interactions, sensory experiences, emotional safety, and responsive feeding shape cognitive abilities, emotional regulation, and long-term health in ways that are hard to reverse.
What shapes the quality of caregiving? Much of it depends on the mental, physical, and social condition of the caregiver. A teenage mother in rural India often faces multiple pressures that would challenge any adult, let alone an adolescent. She may be adjusting to a new household after marriage. She is likely anaemic and physically drained from pregnancy and breastfeeding. She may have dropped out of school. She often lacks control over her own health and diet. She is isolated from her family. She may be dealing with postpartum depression without access to mental health services.
Research on early childhood development, including studies in rural India, consistently shows that maternal stress, depression, and physical exhaustion lower the quality and responsiveness of caregiving. Responsive caregiving means engaging with the child, making eye contact, responding to cries, playing, explaining the world, and creating a sense of safety. These interactions are vital. They are how early brain development occurs. When a mother feels overwhelmed, exhausted or emotionally distant – not by choice, but due to her circumstances, these vital interactions become less frequent and lower in quality. The child receives less stimulation and emotional connection, which are necessary for the developing brain.
Studies in rural Haryana found that many mothers believed young infants were “too young to understand”. This view, while understandable, contradicts scientific evidence that shows adversity affects children in their very first weeks of life. Toxic stress in infancy – stemming from unpredictable, unsupportive environments – is linked to structural changes in the developing brain, which can impact learning, behaviour, and health into adulthood.
This is not a moral criticism of young mothers. It is a structural observation: a sixteen-year-old girl who is anaemic, isolated, uneducated, and unsupported cannot provide the high-quality early caregiving her child’s development needs. This is not about who she is, but rather what opportunities have been denied to her.

The Chain That Links Generations
NFHS-5 allows us to see how this issue affects generations. Children of anaemic mothers are much more likely to be anaemic themselves. The under-five anaemia rate in India is 67.1% in NFHS-5, which rose from 59% in NFHS-4. A mother’s anaemia status is one of the main factors driving childhood anaemia, along with socioeconomic status and educational attainment.
Children born to mothers with lower education levels tend to have higher infant mortality rates. Kids born underweight are more likely to be stunted. Stunted children often have delayed cognitive development. Children with delayed cognitive development perform worse in school. Kids who struggle in school are more likely to drop out early. Girls who drop out early are more likely to marry young.
And those young married girls are more likely to become teenage mothers. The cycle continues. The cycle of disadvantage is not just a metaphor—it is measurable, traceable, and follows predictable paths through the lives of women and children.
What Policy Looks at and What It Misses
India has programs addressing part of this situation. The POSHAN Abhiyan focuses on nutrition throughout life. Anaemia Mukt Bharat provides iron and folic acid supplements. The Beti Bachao Beti Padhao initiative works on girls’ education and survival. The SABLA program targets adolescent girls’ nutrition and life skills. However, several gaps remain.
A girl who is anaemic, out of school, and at risk of early marriage may fall under three different departmental mandates without a single point for coordination. The pathway from anaemia to early marriage to teenage pregnancy to intergenerational stunting is a continuous thread; the policy response is a series of disconnected actions.
They reach girls too late—or not at all. Many interventions target pregnant women or mothers of young children. The critical time when a girl’s own nutrition, education, and life choices are being formed receives relatively less attention and resources. By the time a teenager is pregnant, multiple prior failures have likely taken place.
Mental health is mostly missing from the discussion. Issues like postpartum depression in young mothers, stress for caregivers, and isolation in new households contribute significantly to lower caregiving quality, which negatively affects child development. India’s public health system cannot effectively tackle this problem, especially in rural areas.
The issue of marriage remains politically tricky. While child marriage has decreased nationwide, it still occurs frequently in certain regions. Enforcing current laws and investing in girls’ secondary education is the best way to prevent early marriage. However, this needs ongoing political commitment that data alone cannot provide.
What Supporting a Girl Early Would Actually Look Like
The main idea here is straightforward. Early interventions—before marriage, pregnancy, and childbirth—offer the greatest benefits for both mothers and the children they will raise.
Supporting a young girl means helping her stay in school beyond the primary level, where dropout rates rise. It means making sure she is not anaemic before she gets pregnant. It means postponing marriage until she is an adult. It also means ensuring that when she becomes a mother, she has access to good antenatal care, nutritional help, and some kind of mental support during the months before and after delivery.
None of these actions are extraordinary. They do not require discoveries. There is a wealth of evidence supporting them, which has been available for decades.
What is needed is a policy framework that views teenage girls not as future health statistics, but as individuals whose current situations—education, nutrition, ability to delay marriage, and access to support—will not only influence their own lives but also the future development of the next generation. India’s childhood development outcomes will not improve sustainably until the country’s adolescent girls receive better support. The data clearly shows this. The critical question is whether the policy will take action.
Clear Cut Health, Education Desk
New Delhi, UPDATED: May 26, 2026 09:00 IST
Written By: Muskan Pal

