India’s NCD programmes, especially NPCDCS, remain largely gender-neutral, failing to address women’s unique health risks and barriers. A gender-responsive, life-course approach is essential to improve early detection, access, and outcomes for women.
Non-communicable diseases (NCDs) are responsible for nearly 74% of deaths globally, with India experiencing a rapidly rising burden of cardiovascular diseases (CVDs), diabetes, cancers, and chronic respiratory conditions. While the National Programme for Prevention and Control of Non-Communicable Diseases (NPCDCS) represent a landmark national response, its current design remains largely gender-neutral, overlooking the unique biological, social, and structural determinants affecting women’s health.
Emerging evidence and policy analyses indicate that women in India are often “empowered in rhetoric but excluded in design”, a pattern that extends to NCD programmes. This brief highlights critical gender gaps in NPCDCS and proposes a gender-transformative, life-course approach to strengthen preventive strategies and NCD outcomes among women.
The policy context for NCD control in India is shaped by initiatives such as the NPCDCS, which operates under the National Health Mission (NHM) and prioritizes screening, early diagnosis, and management of major NCDs. Recent health system reforms, particularly Ayushman Bharat and the establishment of Health and Wellness Centres (HWCs), have created significant opportunities for delivering integrated, community-based NCD care at the primary healthcare level. However, despite these advancements, challenges persist in implementation, as gender-responsive budgeting and program monitoring often focus on beneficiary coverage rather than outcome-based impact, thereby limiting the potential for achieving meaningful and transformative improvements in population health outcomes.
Despite strong policy intent, significant gender bias persists across the continuum of NCD care. Women often experience delayed diagnosis and under-recognition of conditions such as cardiovascular diseases, partly due to atypical presentations and systemic gaps in clinical awareness. Existing screening programmes inadequately account for sex-specific risk factors, including pregnancy-related complications and menopausal transitions, which are critical determinants of long-term health. Furthermore, structural barriers, such as time poverty, disproportionate unpaid caregiving responsibilities, and limited decision-making autonomy, continue to restrict women’s access to timely healthcare services. Compounding these challenges, current monitoring systems largely lack sex-disaggregated and outcome-oriented indicators, thereby limiting the ability to assess and address gender inequities effectively within NCD prevention and control strategies.
Key Evidence and Gaps in Gender-Responsive NCD Care
Despite growing recognition of gender disparities in NCDs, substantial evidence highlights persistent gaps across clinical, health system, socio-structural, and data domains. Clinically, the atypical presentation of cardiovascular diseases in women often results in missed or delayed diagnoses, while critical risk factors such as reproductive history, including preeclampsia and gestational diabetes mellitus, remain inadequately integrated into routine NCD risk assessment frameworks. At the health system level, the predominance of facility-based screening models limits outreach to women with restricted mobility, compounded by insufficient provider training in gender-sensitive care.
Socio-structural barriers further exacerbate inequities, as women’s time poverty and disproportionate unpaid caregiving responsibilities reduce health-seeking behaviour, reflecting deeper gender biases in policy design; additionally, urban–rural and socioeconomic disparities widen access gaps. Finally, significant data and accountability deficits persist, including the absence of sex-disaggregated outcome indicators and an overemphasis on financial allocations rather than measurable health outcomes. aligning with broader limitations observed in gender-responsive budgeting approaches.
The NPCDCS reflect strong policy intent; however, its implementation remains largely gender-blind in practice. Current approaches tend to emphasise uniform screening protocols rather than context-specific, tailored strategies that address women’s unique risk profiles. Additionally, there is a predominant focus on coverage- based metrics instead of equity and outcome-oriented indicators, which limits the ability to assess real health gains among women.
Socio-structural barriers further exacerbate inequities, as women’s time poverty and disproportionate unpaid caregiving responsibilities reduce health-seeking behaviour, reflecting deeper gender biases in policy design; additionally, urban–rural and socioeconomic disparities widen access gaps. Finally, significant data and accountability deficits persist, including the absence of sex-disaggregated Outcome indicators and an overemphasis on financial allocations rather than measurable health outcomes, aligning with broader limitations observed in gender-responsive budgeting approaches.
The NPCDCS reflect strong policy intent; however, its implementation remains largely gender-blind in practice. Current approaches tend to emphasize uniform screening protocols rather than context-specific, tailored strategies that address women’s unique risk profiles. Additionally, there is a predominant focus on coverage- based metrics instead of equity and outcome-oriented indicators, which limits the ability to assess real health gains among women.
The NPCDCS reflect strong policy intent; however, its implementation remains largely gender-blind in practice. Current approaches tend to emphasize uniform screening protocols rather than context-specific, tailored strategies that address women’s unique risk profiles. Additionally, there is a predominant focus on coverage- based metrics instead of equity and outcome-oriented indicators, which limits the ability to assess real health gains among women. The absence of intersectional targeting further overlooks the needs of vulnerable groups, including peri-menopausal women and those inunderserved settings. Consequently, these gaps contribute to suboptimal detection, delayed care, and an increased long-term NCDs risk among women, reinforcing existing gender inequities within the NCD care continuum.
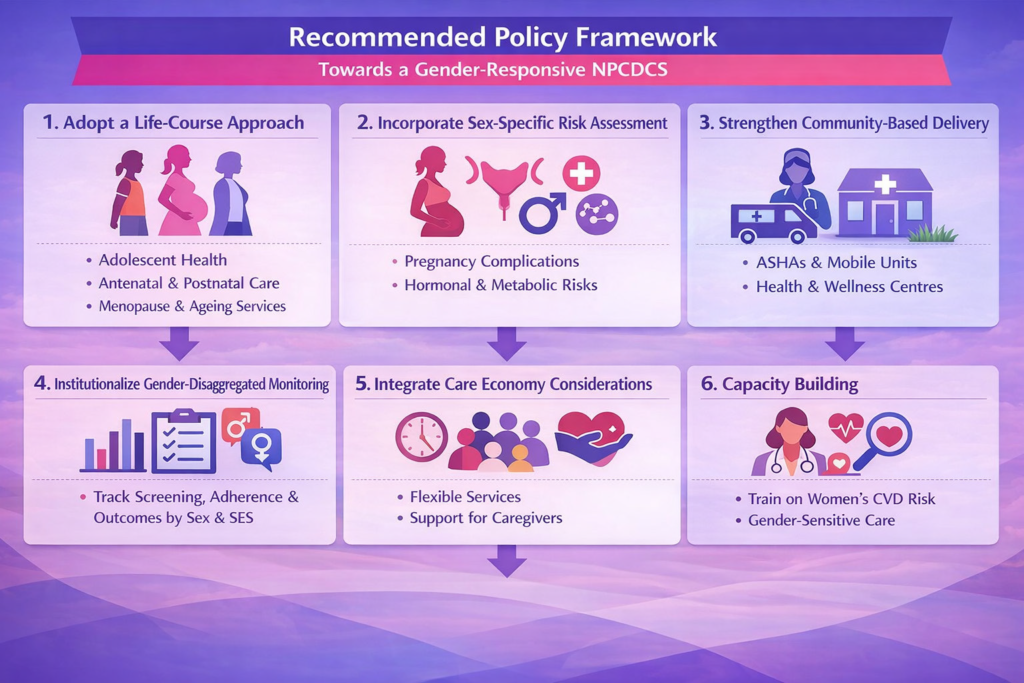
Strategic Recommendations
To advance gender-responsive NCD care, the Government of India should prioritise the establishment of dedicated Women’s NCD Health Units within primary healthcare systems to enable focused screening, early detection, and management. Strengthening alignment between the NPCDCS, Ayushman Bharat, and RMNCH+A is essential to ensure integrated and continuum-based service delivery across
the life course. There is a critical need to shift towards outcome-based gender budgeting, emphasizing measurable health gains rather than solely financial allocations. Additionally, promoting targeted research on women’s NCDs, particularly peri-menopausal cardiovascular risk, will help bridge existing evidence gaps. Enhancing multi-sectoral convergence across domains such as nutrition, sanitation, and social protection can address underlying social determinants of health. Finally, leveraging digital health platforms like the Ayushman Bharat Digital Mission (ABDM) can facilitate real-time,gender-sensitive data collection and surveillance, thereby strengthening monitoring, accountability, and evidence-based policymaking.
Implications for Public Health Practice
Adopting gender-responsive approaches within NCD programmes can significantly enhance public health practice by enabling earlier detection and prevention of cardiovascular diseases among women, particularly those at higher risk. Such strategies can help reduce persistent health inequities across socio-economic groups by improving access to screening, diagnosis, and care.
Additionally, integrating gender-sensitive service delivery within primary healthcare systems can strengthen their responsiveness, efficiency, and overall effectiveness. Collectively, these efforts contribute to achieving broader global health and development goals, particularly SDG 3 (Good Health and Well-being) and SDG 5 (Gender Equality), by promoting equitable and inclusive health care
systems
Conclusion
India stands at a critical juncture in its response to non-communicable diseases (NCDs). While the NPCDCS provides a strong policy foundation, achieving meaningful and sustained impact necessitates a shift from gender- neutral approaches to truly gender- transformative action. From a public health perspective, prioritizing women’s health is not merely an issue of equity but a public health imperative, as it holds significant potential to reduce the overall NCD burden and improve population-level health outcomes across the country.
About the Writer:
Dr. Shazina Saeed is a senior academic at the Amity Institute of Public Health & Hospital Administration, Amity University, Noida, and a qualified Clinician with extensive expertise in non-communicable diseases (NCDs) and preventive cardiology. She holds advanced degrees in Public Health Genetics (MPH) and Clinical Genetics (MS) from the University of Pittsburgh, USA With over 15 years of multidisciplinary experience spanning clinical medicine, public health, and genetics, and a PhD in Clinical Research, she brings a comprehensive and translational perspective to NCD prevention and women’s cardiovascular health. Her work integrates clinical insights with population-level strategies, and she has led and contributed to several research initiatives, including ICMR-funded projects. She also serves as a reviewer and associate editor for multiple reputed international journals, reflecting her active engagement in advancing global health research.
Clear Cut Health Desk
New Delhi, UPDATED: April 16, 2026 05:48 IST
Written By: Dr. Shazina Saeed