Disability in rural India is widespread but underserved, with limited access to physiotherapy and rehabilitation due to infrastructure gaps, stigma, and low awareness. These challenges are further intensified by poverty, distance, and gender inequality, restricting care and social inclusion.
Disability in India is both a public health challenge and a social issue shaped by geography, infrastructure, and deeply embedded cultural beliefs. A significant proportion of persons with disabilities live in rural areas where access to rehabilitation services (particularly physiotherapy) remain limited. Long travel distances, shortage of trained professionals, lack of early diagnosis, inaccessible public infrastructure, and persistent socio-cultural stigma collectively prevent many disabled individuals from receiving consistent care. These challenges are often intensified by gendered norms within patriarchal rural societies, where women with disabilities face greater marginalization in healthcare access, employment, and marriage prospects.
Prevalence & Awareness of Disability in Rural India
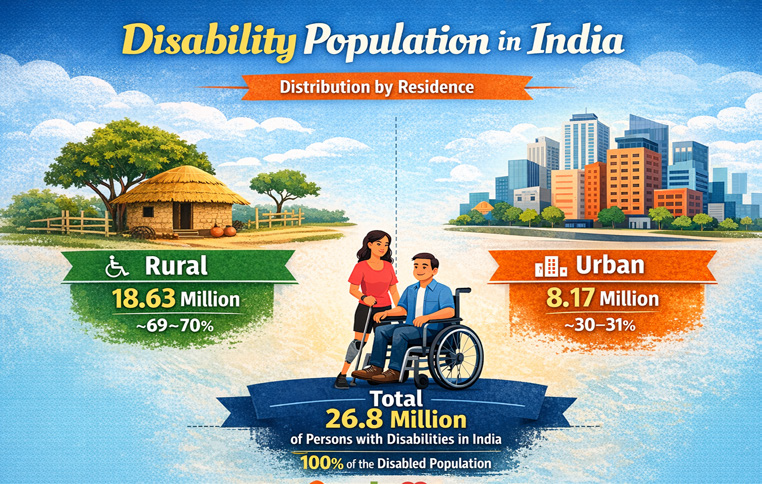
Understanding disability in rural India requires looking at both statistical prevalence and the level of awareness about disability and rehabilitation services within communities. According to the Census of India 2011 conducted by the Office of the Registrar General & Census Commissioner, India, 26.8 million people (2.21% of India’s population) were recorded as living with disabilities. A striking feature of this data is the strong rural concentration: about 18.6 million people with disabilities (nearly 70% of the total) live in rural areas, compared with roughly 8.1 million in urban regions.
This rural dominance is partly explained by India’s demographic structure, where a large share of the population resides outside cities. However, the data also reflects structural disparities in healthcare access, occupational risk, and poverty levels. Rural livelihoods often involve physically demanding work such as agriculture, construction, or manual labour, which increases vulnerability to injuries and long-term musculoskeletal conditions requiring rehabilitation.
Despite the large number of disabled individuals living in villages, awareness about disability identification, rights, and rehabilitation services remains limited. Experts have suggested that the actual number of persons with disabilities in rural areas may be higher than reported because of undercounting linked to social stigma and lack of awareness.
For example, community health workers in several states have reported that families often interpret
disability through cultural or spiritual frameworks, viewing it as fate or divine will, rather than as a medical
condition requiring rehabilitation. As a result, families may delay seeking professional help, especially when services are located far from villages.
Education data also reflects this gap in awareness and access. Government education statistics show that nearly 69% of children with disabilities enrolled in schools come from rural areas, highlighting both the concentration of disability in villages and the continuing challenges of inclusive education and rehabilitation support systems.
Age also influences disability prevalence. Research based on census data shows that disability rates increase significantly with age, particularly among those over 60 years. In rural India, where access to preventive healthcare is limited and occupational injuries are common, elderly individuals are especially
vulnerable to mobility impairments.
Taken together, these patterns highlight a clear reality: disability in India is predominantly a rural phenomenon, yet awareness and rehabilitation services remain disproportionately urban. Addressing this gap is essential for improving both health outcomes and social inclusion for millions of rural residents living with disabilities.
Social Stigma and Cultural Barriers
Disability in rural India is shaped not only by medical conditions but also by deeply embedded social perceptions and cultural attitudes. Stigma often emerges from the way disability is understood within communities – as a misfortune, a burden on the family, or even a result of fate or past actions. These interpretations can discourage families from seeking medical care or rehabilitation services, particularly
in the early stages of disability.
Studies in the field of disability and public health suggest that stigma contributes to underreporting of disabilities, especially in rural communities, where families may hesitate to disclose a member’s condition due to fear of discrimination or social exclusion.
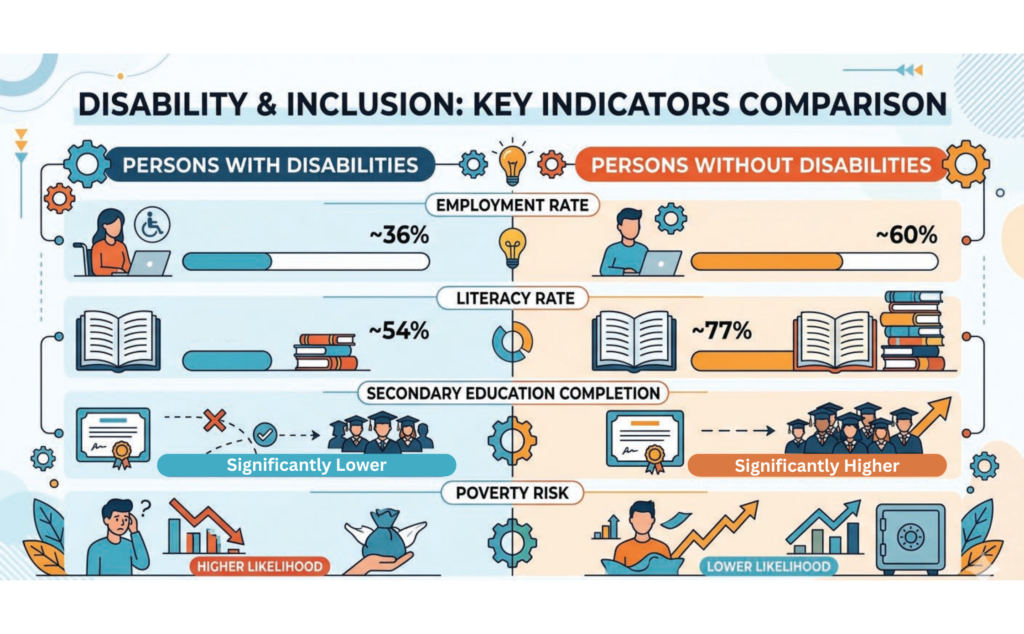
Evidence from the World Health Organization indicates that people with disabilities worldwide are more
likely to experience social isolation, lower education levels, and reduced employment opportunities. These
trends are particularly visible in rural India. Data from the National Sample Survey Office show that persons with disabilities have lower workforce participation rates compared with the general population, reflecting both structural barriers and social attitudes that limit opportunities.
In states such as Uttar Pradesh and Bihar, community health workers have reported cases where families initially seek traditional or faith-based remedies before approaching medical professionals for rehabilitation. Such delays can significantly affect long-term recovery outcomes, especially in conditions that benefit from early physiotherapy intervention.
Social stigma also influences mobility and visibility in public spaces. Individuals with physical impairments often face challenges participating in community events, employment, or education due to both physical inaccessibility and social attitudes that perceive disability primarily through a lens of dependency. As
a result, many disabled individuals remain largely invisible within village public life.
Patriarchy & Gendered Experiences
Disability in rural India often intersects with entrenched patriarchal norms, shaping markedly different experiences for men and women. While disability itself can restrict mobility, education, and employment, women with disabilities frequently face double discrimination, both as women and as persons with disabilities. According to the Census of India 2011 compiled by the Office of the Registrar General & Census Commissioner, India, men constitute a larger proportion of the reported disabled population than women. Researchers suggest that this gap may partly reflect under reporting of disability among women, as families may hesitate to disclose a daughter’s disability due to concerns about social stigma and marriage prospects.
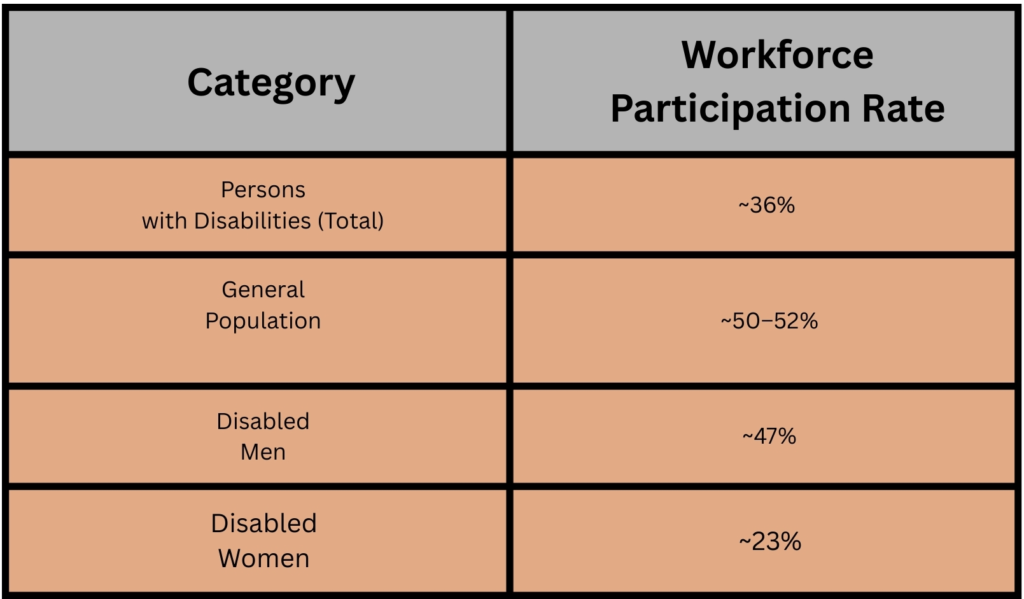
Employment data further highlights this gender disparity. Analysis by the National Statistical Office indicates that labour force participation among women with disabilities is significantly lower than that of men with disabilities, reflecting barriers related to mobility, education, and cultural expectations about
women’s roles within the household.
In rural communities, patriarchal norms often prioritise healthcare for male family members, especially
when resources are limited. Women with disabilities may therefore receive delayed diagnosis, irregular
physiotherapy treatment, or limited access to rehabilitation services. Social expectations around marriage also play a significant role: while disabled men may still be considered eligible for marriage, disabled women often face rejection or pressure to remain economically dependent on their families. These gendered experiences highlight the need for disability policies and rehabilitation programs that explicitly
address patriarchal barriers, ensuring equitable access to healthcare, education, and social participation
for women with disabilities.
Diagnosis & Treatment Protocols
Effective disability care depends heavily on timely diagnosis and structured rehabilitation protocols.
In rural India, however, these processes are often fragmented. Limited availability of specialists, low
awareness among families, and weak referral systems frequently delay diagnosis and treatment. As a
result, many conditions that could be managed or improved through early physiotherapy interventions
progress into long-term disabilities. Early identification of disability is critical for preventing functional deterioration and improving long-term outcomes.
Conditions such as cerebral palsy, developmental delays, stroke-related impairments, spinal injuries, and musculoskeletal disorders require early screening and timely intervention. However, access to diagnostic facilities remains uneven across rural India. Data from the National Sample Survey Office indicates that a
large proportion of persons with disabilities in rural areas are diagnosed later in life, often after symptoms significantly affect mobility or daily functioning. In children, delayed diagnosis can affect cognitive and motor development. For example, children with developmental conditions may not be identified until they enter school, by which time valuable early intervention windows may have passed.
Government initiatives such as the Rashtriya Bal Swasthya Karyakram (RBSK) were introduced to improve early detection of developmental delays and disabilities among children through school and community screening. However, implementation remains uneven across rural districts due to shortages of trained medical personnel and limited awareness among families.
Physiotherapy plays a vital role in the rehabilitation of individuals with physical disabilities. Through targeted exercises, mobility training, and pain management techniques, physiotherapy helps restore functional independence and prevent complications such as muscle stiffness, joint contractures, and chronic pain.
The World Health Organization recognizes rehabilitation, including physiotherapy, as an essential component of universal health coverage. For conditions such as stroke, spinal cord injuries, fractures, and neurological disorders, early physiotherapy significantly improves recovery outcomes and quality of life. In rural India, however, physiotherapy services are largely concentrated in urban hospitals and private clinics. Many primary health centres lack dedicated rehabilitation professionals, forcing patients to travel to district hospitals for therapy sessions. This geographic imbalance creates barriers to consistent treatment, particularly for individuals who depend on daily wages or family caregivers for travel.
Several systemic gaps continue to limit effective rehabilitation in rural India. First, there is a shortage of trained physiotherapists in rural healthcare facilities. Most physiotherapy professionals work in urban hospitals or private clinics, leaving rural populations underserved. Second, referral systems between primary healthcare centres and rehabilitation specialists are often weak. Patients may receive initial medical treatment but are not systematically referred for physiotherapy or long-term rehabilitation.
Third, rehabilitation protocols are not always integrated into routine healthcare services. While policies
recognise the importance of disability care, many rural health facilities focus primarily on acute medical treatment rather than long-term r e h a b i l i t a t i o n .
These gaps result in delayed recovery, reduced mobility, and increased economic and social burdens for families. Strengthening diagnostic systems, integrating physiotherapy into primary healthcare, and improving referral pathways are therefore essential for building an effective rural rehabilitation framework.
Transportation, Accessibility, & Architectural Barriers
Access to rehabilitation services in rural India is shaped not only by medical availability but also by physical infrastructure. Transportation systems, road conditions, and the design of public spaces significantly influence whether persons with disabilities can reach healthcare facilities, schools, and workplaces. Even when physiotherapy services exist in district hospitals or rehabilitation centres, reaching them regularly can be difficult for rural patients.
Transportation costs, long travel distances, and inaccessible public infrastructure often interrupt treatment schedules and reduce the effectiveness of rehabilitation.
Transportation remains one of the most commonly reported barriers for persons with disabilities seeking healthcare. According to the National Sample Survey Office report on disability in India, a large proportion of persons with disabilities in rural areas depend on family members or private transport to access medical services, as accessible public transportation options are limited. The survey also found that over one-third of persons with disabilities reported difficulties in reaching healthcare facilities, particularly in rural regions where medical services are often located far from villages.
Distance itself can become a major obstacle. Rural patients frequently travel 20–50 kilometres to reach district hospitals or rehabilitation centres, where physiotherapy services are typically available. For daily wage labourers or low-income families, the cost of repeated travel combined with lost workdays makes regular therapy financially challenging.
Beyond transportation, the physical design of public infrastructure often restricts mobility for persons with disabilities. Many rural health centres, government offices, schools, and public buildings lack basic accessibility features such as ramps, handrails, wide doorways, or accessible toilets.
The Accessible India Campaign launched by the Government of India aims to improve accessibility in public infrastructure across the country. However, progress has been uneven, particularly in rural areas where older buildings were constructed without universal design principles.
Inaccessible infrastructure can discourage disabled individuals from seeking care or participating in community life. For instance, a patient using a wheelchair may find it difficult to enter a rural clinic if the building has steps but no ramp. Similarly, narrow corridors or crowded waiting areas can make mobility challenging for individuals using assistive devices such as walkers or crutches.
Such architectural barriers reinforce social exclusion by limiting independent access to healthcare, education, and public services. Addressing these issues requires incorporating universal design standards into rural infrastructure development, ensuring that accessibility becomes a core element of healthcare planning rather than an afterthought.
Social & Healthcare Investment
Improving disability care in rural India requires sustained investment not only in medical infrastructure but also in social systems that support rehabilitation and long-term inclusion. While policy frameworks addressing disability have expanded over the past decade, the allocation of resources and implementation of services remain uneven across rural regions. Strengthening healthcare investment, community participation, and public awareness is therefore critical for improving access to physiotherapy and rehabilitation services.
Government expenditure on healthcare in India has gradually increased but still remains relatively low compared to many other countries. According to the National Health Authority and budget data from the Government of India, public health expenditure reached around 2.1% of GDP in 2022–23, with a national goal of increasing it to 2.5% of GDP by 2025. Although this expansion aims to strengthen healthcare infrastructure, rehabilitation services, including physiotherapy, often receive limited dedicated funding within rural healthcare systems.
Programs under the National Health Mission have helped expand primary healthcare facilities in rural areas, including sub-centres, primary health centres, and community health centres. However, most of these facilities focus primarily on maternal health, infectious diseases, and emergency care. Rehabilitation services such as physiotherapy are still rarely integrated as routine services within these institutions. Investment in disability-specific welfare programs has also grown through initiatives such as the Unique Disability ID (UDID) Scheme and financial assistance for assistive devices under schemes implemented by the Department of Empowerment of Persons with Disabilities. These programs aim to streamline disability certification and improve access to government benefits. Yet in many rural areas, awareness about these schemes remains limited, and bureaucratic processes can delay access to assistance.
Community participation plays a crucial role in bridging these gaps. Village health committees, local self-help groups, and grassroots health workers, such as Accredited Social Health Activists (ASHAs), often act as intermediaries between families and healthcare systems. By raising awareness about rehabilitation services, facilitating disability certification, and guiding families toward physiotherapy care, these community actors can significantly improve access to support.
Expanding social and healthcare investment therefore requires a dual approach: strengthening institutional infrastructure while simultaneously empowering local communities to participate in disability inclusion and rehabilitation efforts.
The Future Role of Physiotherapy in Rural India
As India’s rural healthcare system continues to evolve, physiotherapy is increasingly recognized as a critical component of comprehensive medical care. Traditionally, rural healthcare has focused on infectious diseases, maternal health, and emergency treatment, while rehabilitation services have received comparatively little attention. However, demographic changes, rising life part of long-term healthcare planning.
According to the World Health Organization, the global demand for rehabilitation services is growing rapidly due to aging populations and increasing chronic health conditions. In India, these trends are especially significant in rural areas, where healthcare infrastructure is already under strain and access to specialized services remains limited.
Physiotherapy can play a transformative role in rural healthcare by addressing mobility impairments, reducing pain, and helping individuals regain independence in daily activities. For patients recovering from fractures, neurological disorders, or musculoskeletal injuries, regular physiotherapy can prevent long-term disability and improve quality of life. Integrating physiotherapy services into primary healthcare centres could therefore significantly reduce the rehabilitation gap between urban and rural populations. One promising direction is the expansion of community-based rehabilitation (CBR) programs, which train local health workers and caregivers to assist with basic physiotherapy exercises and mobility training at home. This approach is particularly effective in rural settings where travel to hospitals is difficult and continuous therapy is required over extended periods.
Technological innovations are also opening new possibilities. Tele-rehabilitation platforms allow physiotherapists in urban hospitals to remotely guide patients and local healthcare workers through treatment routines using smartphones or digital health applications. With India’s growing digital connectivity, such models have the potential to extend rehabilitation services to remote villages where physiotherapists are scarce. At the same time, expanding physiotherapy education and encouraging graduates to work in rural healthcare systems will be crucial. Government incentives, rural service programs, and partnerships between medical colleges and district hospitals could help distribute
rehabilitation professionals more evenly across the country.
Ultimately, the future of physiotherapy in rural India lies in integration, innovation, and inclusion, integrating rehabilitation into primary healthcare systems, innovating through technology and community
programs, and ensuring that physiotherapy services reach the populations that need them most.
In a country as vast and diverse as India, equitable rehabilitation will require sustained commitment. Yet The potential impact is profound: restoring mobility, independence, and dignity to millions of people whose lives—and futures—depend on access to care.
About the Writer:
A research scholar in Manipal Institute of Technology, Manipal, currently exploring Earth’s processes and the evolving human footprint in the fragile Himalayan landscape.
Clear Cut Health Desk
New Delhi, UPDATED: April 21, 2026 02:06 IST
Written By: Antara Mrinal